Being Black in America Is a Health Risk. It’s Time for Reparations.
Credit to Author: Jason Silverstein| Date: Wed, 19 Jun 2019 14:55:11 +0000
On Wednesday, Juneteenth, the day that commemorates the news of the legal end of slavery, Congress will hold the first hearing on reparations for Black Americans since 2007. The idea of reparations for slavery and state-sanctioned discrimination has resurfaced recently, as Trump’s 2020 challengers weigh in on the importance of our country acknowledging, compensating, and correcting racial injustice.
But it’s far from a new idea. There has long been a call for economic justice for the harm of slavery, from post-Civil War attempts to distribute 40 acres and a mule and pensions to formerly enslaved people to, more recently, writer Ta-Nehisi Coates’ landmark 2014 Atlantic essay, “The Case for Reparations.” A bill called H.R. 40, or The Commission to Study and Develop Reparations Proposals for African-Americans Act, has been introduced in Congress every year since 1989 but has never been voted on. It’s this bill that will be discussed in Wednesday’s hearing, in front of the House Judiciary Subcommittee on the Constitution, Civil Rights and Civil Liberties.
While history offers ample justification for reparations, there’s an especially undeniable set of circumstances that illustrate the need to move forward with H.R. 40: Black people in the United States have, since slavery, been systematically overexposed to health risks while also being deprived of healthcare. This lethal combination continues to cause suffering and death, as well as a massive and measurable loss of wealth, because it is expensive to be sick in the U.S.
A healthcare-specific argument for reparations, then, should not be controversial. Public policies have made generations of Black people sick, and those losses ought to be paid back, in cash. Arguments for reparations are often dismissed by detractors who say they personally can’t explain how reparations would work and therefore, by some failure of logic, conclude no one possibly can.
But H.R. 40 could set out to calculate how much families have lost, from hospital charges to days of missed work, and arrive at a dollar amount that Black Americans are owed—unless Congress decides they would rather not know the answer.
It’s not hard to put numbers to this.
The disparities by the numbers
There’s no denying that being Black in America is a health risk. Racial health disparities have been extensively documented when it comes to asthma, arthritis, aggressive breast cancer, kidney disease, heart failure, maternal mortality, lung disease, chemical exposures, and overall life expectancy.
“Racial health disparities have existed as long as medicine has existed in this country,” said Brian Smedley, executive director of the National Collaborative for Health Equity.
The persistence of these disparities is astounding. In 1896, the sociologist W.E.B. Du Bois showed that Black children under five were three times more likely to die than white kids; today, Black infants are still twice as likely to die as white babies. In 1915, Booker T. Washington estimated that 45 percent of Black deaths were completely preventable. Nearly 100 years later, Robert Wood Johnson Foundation Health and Society Scholars investigated why so many more Black Americans die before they turn 65 than white Americans. They found that 70 percent of the gap in early deaths was from treatable conditions like diabetes, high blood pressure, and appendicitis.
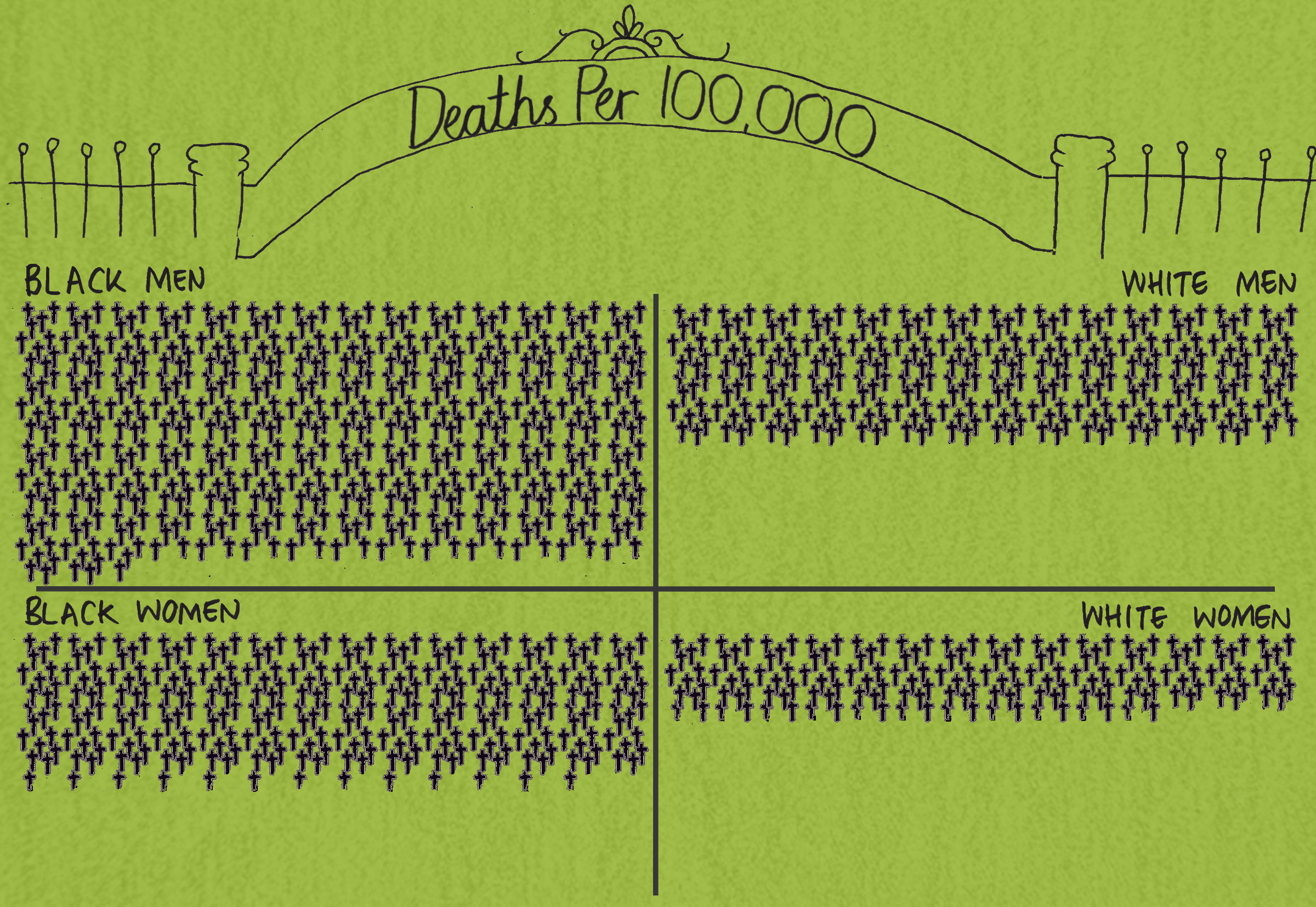
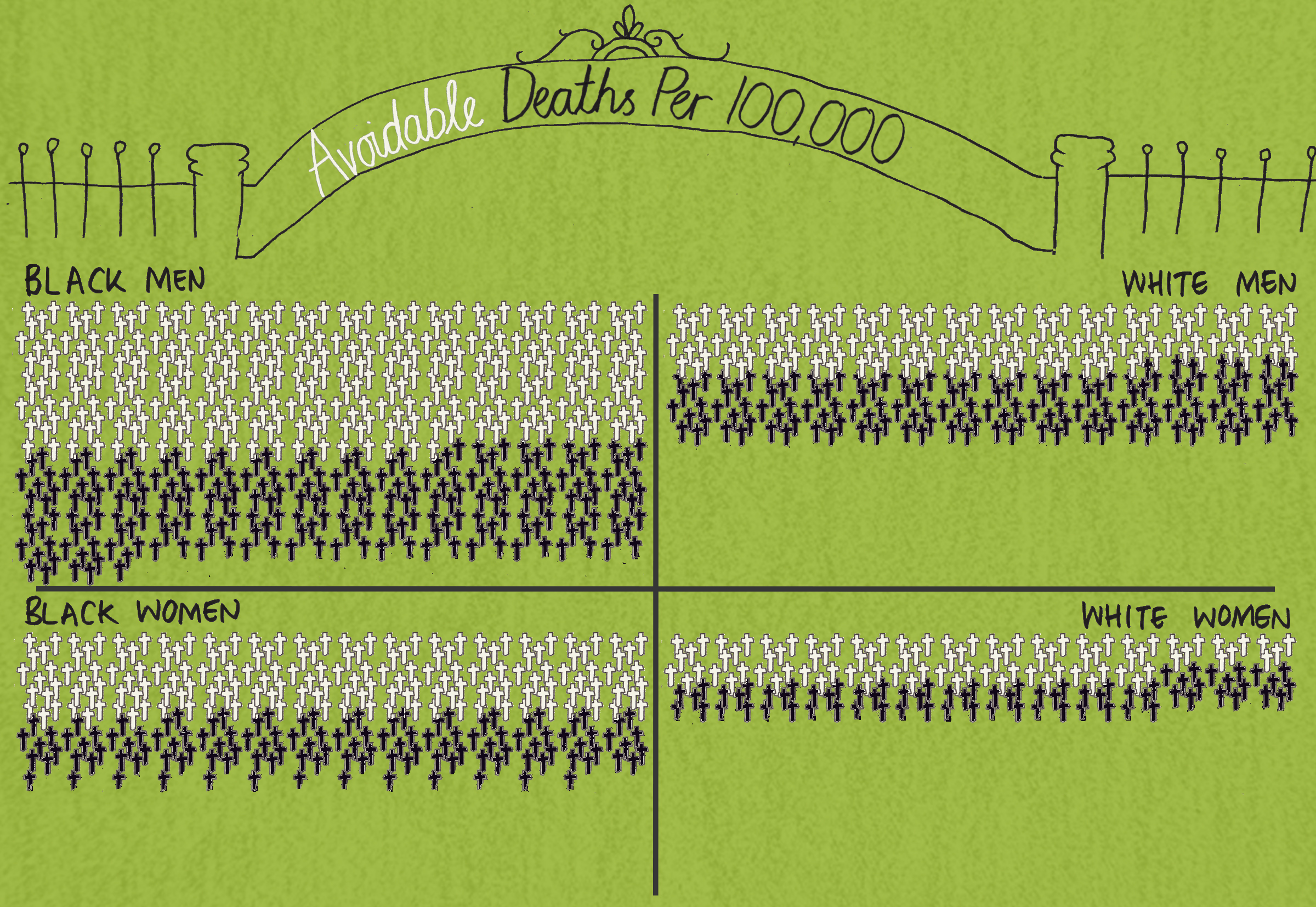
How many people have died from racial health disparities? In 2005, David Satcher, the former surgeon general, and colleagues, published an analysis of 40 years of death rates using data from the National Center for Health Statistics. In 1960, racial health disparities took the lives of more than 60,000 Black Americans. By 2000, the number had reached nearly 84,000. While the number of people dying from racial disparities has decreased since the early 2000s, let’s put this into perspective: For decades, the number of people dying from racial health disparities in the U.S. was even higher than the number dying from opioid overdoses today—yet only one of these crises was ever splashed all over the media and designated a national emergency.
You don’t have to go too far into the past to find the underlying causes of these health disparities
From the Middle Passage to slave labor camps to Jim Crow to the present, at the root of these disparities is segregation, which, as a matter of public policy, sorted Black people into places that incubate illness. The effect, according to Rodney Hood, the former president of the National Medical Association, in a 2001 column on reparations, has been to repeatedly lock Black people into “contagious, cruel, and stressful” environments while also locking them out of healthcare.
Mary Anne Adams is a 64-year-old Black woman who was born during the reign of Jim Crow in Oxford, Mississippi. The South that Mary Anne was born into by law restricted Black people from receiving healthcare. Jim Crow laws segregated hospitals in Mississippi and made it illegal for nurses to treat Black men in Alabama. One out of three hospitals in the South would not treat Black people even in emergencies, according to a study published the year after Mary Anne was born.
Though Mary Anne was one of 10 children, none were born in hospitals—indeed, fewer than 10 percent of all Black infants were born in hospitals in Mississippi at that time. “I have no recollection of Black women going to a hospital to give birth,” Adams said.
The outcome is what you would expect: Before the federal government forced desegregation in hospitals, more than six times as many Black babies were dying of diarrhea and pneumonia than white infants in Mississippi.
Meanwhile, in St. Louis, Missouri, a series of conscious policy decisions segregated the city, ultimately creating an 18-year Black-white disparity in life expectancy. As VICE has previously reported, the real estate industry put an enormous amount of blood, sweat, and white tears into this effort, starting with a 1916 racial zoning ordinance, which kept Black people from moving onto blocks that were mostly white. When the Supreme Court ended the ordinance, industry leaders turned to racial deed covenants, which said white home buyers couldn’t rent to Black people. When the courts stopped them from using those covenants, they created residential security maps, which allowed lenders to deny Black people mortgages on the basis of “undesirability” or other less overtly racist-sounding euphemisms. This practice, known as redlining because of the red colour applied to the “undesirable” areas on maps, resulted in only 3.3 percent of Black people in St. Louis having mortgages by the early 1960s.
The result of these and other practices, such as designing highways that cut off Black neighbourhoods, has been to trap Black people in places with greater exposure to environmental threats like air pollution and lead poisoning, while cutting off access to social goods like quality food and pharmacies.
Not only do these environments lead to Black communities facing higher rates of health problems, but at every step of the healthcare-seeking process, Black people run into man-made barriers: There are often fewer choices of providers in their communities, transportation barriers to seeing those providers, and higher costs to get the care needed. Even if people can clear those hurdles, there’s a risk of not receiving the same quality treatment as white patients for the same conditions, too often with deadly consequences.
For example, people with aggressive prostate cancer need surgery or a combination of radiation and hormone therapy. “Our data show that Black men with this form of prostate cancer are less likely to get any treatment in such circumstances,” said Quoc-Dien Trinh, an assistant professor of surgery at Harvard Medical School. “If Black men don’t get treated when they have lethal cancer, then obviously they will appear to die more often from this form of cancer.”
Exactly how much do Black people pay?
Since the nation has been indifferent toward the human cost of these racial health disparities, scholars have tried to provoke concern by calculating their financial cost.
“We believe that policy makers should be motivated by the social justice argument, however for some that’s not enough,” said Darrell Gaskin, director of the Johns Hopkins Center for Health Disparities Solutions. “We wanted policymakers to know that injustice comes with a hefty price tag.”
The price tag Gaskin and colleagues calculated totaled $45.3 billion in healthcare costs and another $9.6 billion in lost wages for Black Americans in 2009 alone. While insurance covered an estimated 40 percent of those healthcare costs, Black people spent a staggering $12.5 billion out of pocket in just one year because of racial health disparities.
“It’s a combination of both the direct and indirect costs of medical care,” said John Ayanian, professor of medicine and director of the Institute for Healthcare Policy and Innovation at the University of Michigan. “If conditions like diabetes or asthma or high blood pressure are not diagnosed early, those conditions will worsen and people will develop more complications, and those complications can cause significant direct medical costs—particularly if people are uninsured or underinsured.”
“There are also substantial indirect costs, when people have to take time off from work because they or a family member is ill or losing a job because of their health,” Ayanian said.
Black women with breast cancer, for example, are five times as likely to lose their private insurance and more than twice as likely to lose their jobs than white women with breast cancer. One reason, according to Jenny Spencer of the University of North Carolina at Chapel Hill, is that the “time cost” of cancer is different for Black women. “Black women may be disproportionately likely to have jobs that do not offer flexibility in hours or paid sick leave,” Spencer said. In North Carolina, women also often have to drive a long distance or pay for a taxi or bus to get to a cancer clinic.
When Louise Tatum, of the South Side of Chicago, was first diagnosed with breast cancer, she felt failed by her community hospital, which lost her records and sent letters to the wrong doctor. Tatum, who is Black, travels an hour each way in a shared van for daily radiation treatments. A half-hour procedure is turned into a two-and-a-half hour journey at least, a consequence of how segregation puts distance between people and the services they will die without. “I almost urinated twice in the van, because no one would drop me off,” she said of one recent trip.
Since she started treatment, Tatum has lost her job. “There are not many things I can do,” she said. “I have swelling where I had my surgery and now I have radiation every single day. I haven’t had income since October.”
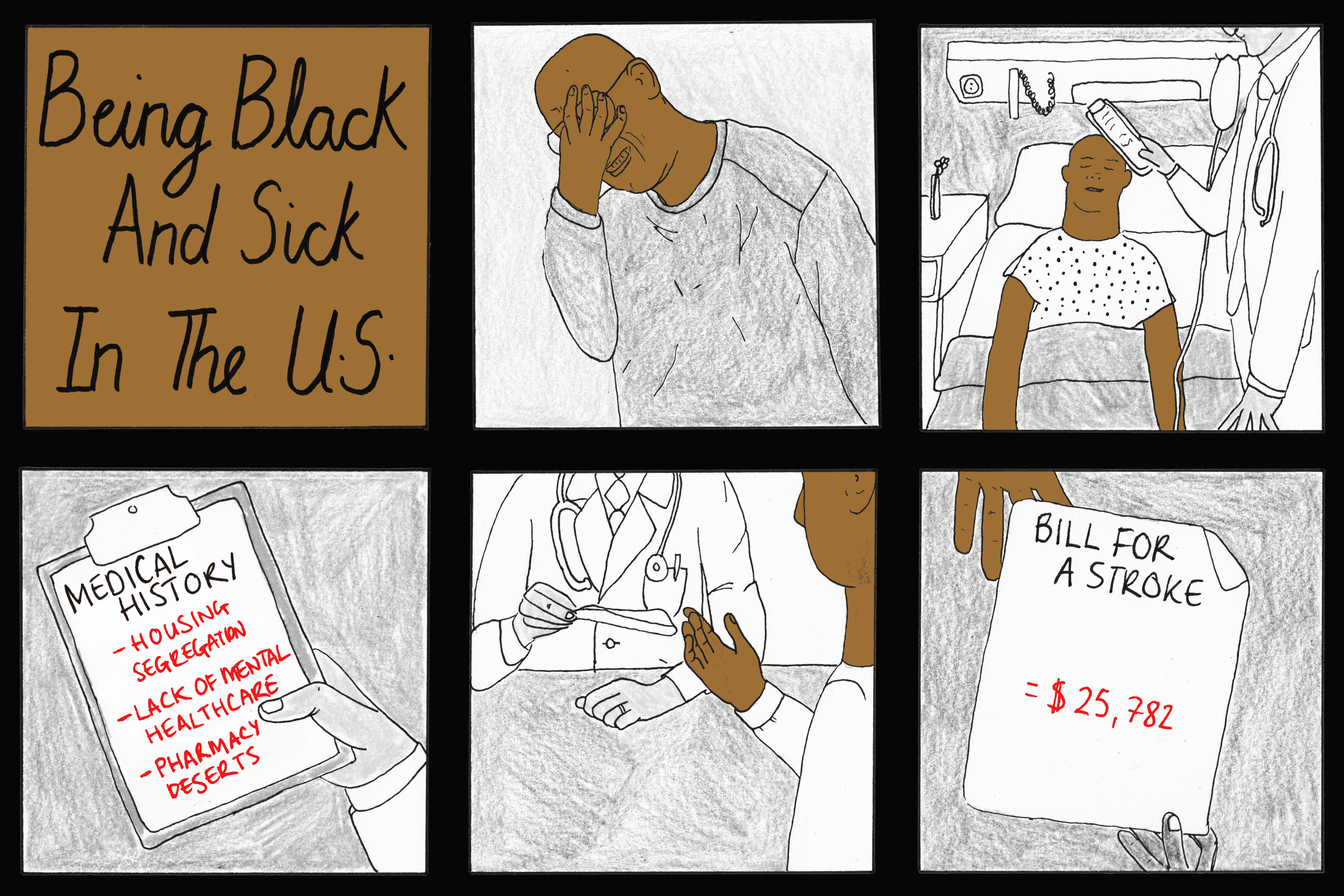
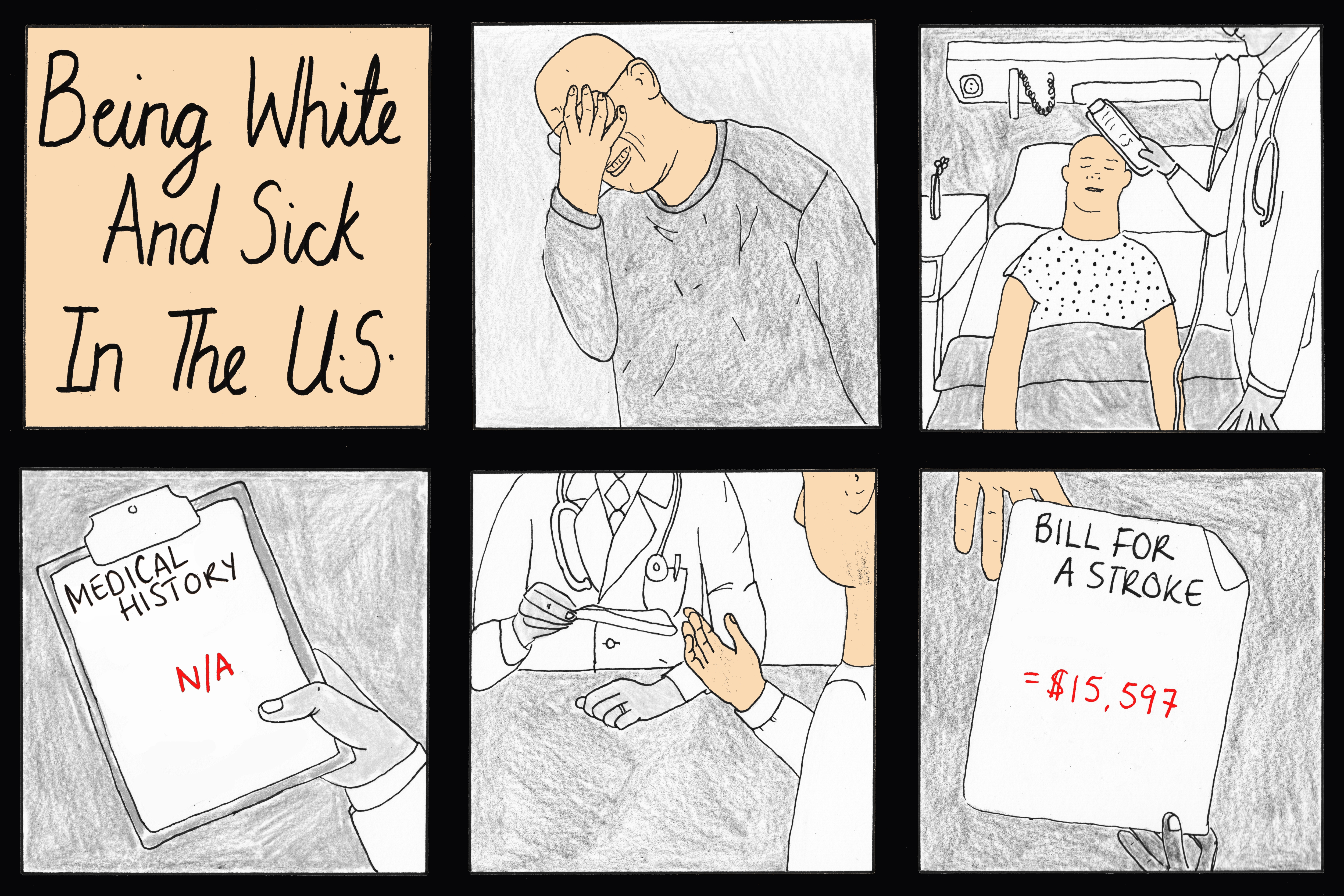
Black people individually pay a staggering price for health disparities, both because of how much they lose when they are sick, like Tatum, and how much more they have to pay because their disease is often much worse by the time they get care. Take the racial disparity in stroke: when a Black person has a stroke, they face an average cost of $25,782, while white people with the same condition are looking at $15,597. Black people pay roughly the same $10,000 racial tax for heart failure ($82,929 vs. $73,985).
Or consider that Black children more frequently need to visit the emergency room for asthma attacks—at an average cost of $2,116, according to Medical Expenditure Panel data—since they’re at greater risk of not having a primary care provider than white children. In Chicago alone, Respiratory Health Association researchers found that Black kids were five times as likely as white kids to visit the ER and determined that preventable charges totaled $6.1 million annually. That doesn’t include the costs of missed days of school and childcare.
Two of Rolinda Robinson’s daughters suffered from severe asthma attacks. Living in the Austin area of the West Side of Chicago, Robinson often drove her children nearly a half hour in the middle of the night to an emergency room she trusted, only to wait two or three hours to be seen. “We would be sitting in the emergency room until the next day to the point where I would be so drained that I could not go to work the next day, as well as she would be so sick that she would not be able to go to school or daycare,” Robinson said.
Though Robinson had health insurance for most of her children’s lives, her insurance did not cover all of the expenses that come with being a single parent trying to care for children with asthma. “There was the constant cost of going back and forth to ER, the gas to get there, paying for parking, and missing time off work,” she explained.
One of the straightest lines we can draw between a racial health disparity and lost wages is lead poisoning. For at least 20 years, it has been known that Black children are at a much greater risk of lead poisoning, a clear consequence of housing segregation that exposes them to lead-based paint and contaminated soil and water.
Lead poisoning has a destructive effect on health, which directly affects a person’s lifelong ability to make money: Children endure behavioral and cognitive problems that may hinder their chances at doing well in school and on tests. “There is strong evidence that exposure to lead in early childhood negatively affects a developing brain and has long-term negative effects on both cognitive achievement and behavior,” said Anna Aizer, an associate professor of economics and public policy at Brown University. “These children will grow up to earn less in adulthood.”
Elise Gould of the Economic Policy Institute estimates that a loss of one IQ point from lead poisoning may lead to a loss of more than $22,000 in lifetime earnings (adjusting for inflation). Now consider that 14 percent of the children poisoned in Flint, Michigan, had very high blood lead levels—above 10 micrograms, which works out to a lifetime loss of at least $162,800 in earnings per child. It is medically impossible to reverse the damage done to the nervous systems of these children. But it is very possible to compensate them for unnecessary harm.
Improving the financial health of Black Americans is critical for improving their mental and physical health
Cash is certainly not an on-off switch to fix racial health disparities (especially maternal mortality, which affects every socioeconomic class of Black women), nor can any amount of money make right the loss of so many lives. Yet, there is evidence that cash reparations would not only be a just form of repayment, but a massive evidence-based health intervention.
Public health scholars David Williams and Chiquita Collins have shown that improving the financial health of Black Americans is critical for improving their mental and physical health. When the racial economic gap was narrowed between 1968 and 1978, so too narrowed the racial health gap (this trend reversed with the widening economic gap in the 1980s).
Both Julián Castro and Elizabeth Warren have endorsed H.R. 40. Cory Booker said he will introduce a companion bill in the Senate; Kamala Harris, Bernie Sanders, and Beto O’Rourke all said they would sign it if they become president. Some candidates support reparations but have crossed out the cash payment option: Pete Buttigieg said he isn’t in favor of direct cash transfers; neither is Bernie Sanders, who said we need a solution other than “just writing out a check.” While former Vice President Joe Biden has not endorsed H.R. 40, Kate Bedingfield, his Deputy Campaign Manager and Communications Director, said Biden “believes that we should gather the data necessary to have an informed conversation about reparations, but he has not endorsed a specific bill.”
The healthcare case for reparations is about, as Kamala Harris argues, “the effects of generations of discrimination and institutional racism” on public health outcomes. (Harris has suggested reparations in the form of trauma treatment and mental healthcare, though she stopped short of endorsing cash payments to families.)
And reparations is also not about taking something away from white people to pay Black people. “Slavery was a federal and state institution,” explained Texas Congresswoman Sheila Jackson Lee, the sponsor of H.R. 40. “I am not going to ask my neighbor who may happen to be white for a check. I am not interested in a check from individuals. I am interested in institutions who created the framework for this elongated period of slavery.”
Martin Luther King, Jr., in his case for reparations, argued that “special measures for the deprived have always been accepted in principle,” and suggested an analogy to the G.I. Bill of Rights for Black people and others who have been disadvantaged—one that would compensate with advantages in school, loans, jobs, and, yes, a check.
Such has been the approach to reparations in Chicago, where, in 2015, the city council voted to give $5.5 million to survivors of police torture, along with health services, job training and placement, college tuition, small business assistance, a permanent memorial, and a class on reparations to eighth-through-tenth grade students.
“No amount of gold could provide an adequate compensation for the exploitation and humiliation of the Negro in America down through the centuries,” King wrote. But however you calculate it, a price can be placed on health disparities—and paid with interest.
Jason Silverstein is a lecturer and writer-in-residence in the department of global health and social medicine at Harvard Medical School.
Sign up for our newsletter to get the best of VICE delivered to your inbox daily.
This article originally appeared on VICE US.